


Cath Lab Spotlight: The Christ Hospital Health Network
Tell us about your facility and cath lab.
 The Christ Hospital Health Network is a 555-bed acute care hospital. The organization operates more than 100 physician offices and outpatient centers throughout the Greater Cincinnati Northern Kentucky area. Our cardiac cath lab and interventional radiology department consists of 5 cath lab rooms, 1 interventional radiology room, and 1 hybrid OR room. We also have a 28-bed holding area for pre and post procedure patients.
The Christ Hospital Health Network is a 555-bed acute care hospital. The organization operates more than 100 physician offices and outpatient centers throughout the Greater Cincinnati Northern Kentucky area. Our cardiac cath lab and interventional radiology department consists of 5 cath lab rooms, 1 interventional radiology room, and 1 hybrid OR room. We also have a 28-bed holding area for pre and post procedure patients.
Our cath lab is part of the Heart and Vascular Service Line, consisting of the Cath Lab and Interventional Radiology, Cardiovascular Recovery Unit (CVRU), Electrophysiology (EP), Cardiovascular Testing Centers (inpatient and outpatient), Cardiovascular Intensive Care Unit (CVICU), Cardiovascular Stepdown Unit (CVSU), 6 South (medical cardiology) and 7 South (heart failure/telemetry), Heart Station, Cardiac Rehab, and Wound Care Center.
What is the size of your department and number of staff members?
 Our department consists of 7 procedural rooms, including 5 cath lab rooms (3 are Philips Allura Xper FD10 and 2 are Philips Allura Xper FD20) for diagnostic and interventional coronary and peripheral procedures, 1 interventional radiology room (Allura Xper FD20), and 1 hybrid OR room (Allura FD20 FlexMove). We also have a dedicated pre and post recovery unit.
Our department consists of 7 procedural rooms, including 5 cath lab rooms (3 are Philips Allura Xper FD10 and 2 are Philips Allura Xper FD20) for diagnostic and interventional coronary and peripheral procedures, 1 interventional radiology room (Allura Xper FD20), and 1 hybrid OR room (Allura FD20 FlexMove). We also have a dedicated pre and post recovery unit.
We average 9.2 years of experience among our staff that consists of a mix of registered nurses (RNs) (30), radiologic technologists (RTs) (25), one clinical coordinator (RN), and 1 interventional cardiology nurse practitioner (NP) to staff the department daily. Five staff members currently have their registered cardiovascular invasive specialist (RCIS) certification, with more staff working on it for this coming year. Our cath labs are open 7:00am–9:00pm, Monday through Friday. Saturday and Sunday are used with on-call staff. Our recovery room is staffed with 12 full-time and 13 part-time RNs. The CVRU department is open Monday through Friday from 5:00am–9:30pm.
Who manages your cath lab?
 The Heart and Vascular Service Center has two directors that include Executive Director Julie Miksit, RN, BSN, MBA, FACHE, and Executive Clinical Director Erik Martin, DNP, RN, CENP. Our Cath Lab and Interventional Radiology Manager is Mary Wagner, RN, BSN, NE-BC, and the Assistant Manager is Bridget Spinney, BRST RT(R).
The Heart and Vascular Service Center has two directors that include Executive Director Julie Miksit, RN, BSN, MBA, FACHE, and Executive Clinical Director Erik Martin, DNP, RN, CENP. Our Cath Lab and Interventional Radiology Manager is Mary Wagner, RN, BSN, NE-BC, and the Assistant Manager is Bridget Spinney, BRST RT(R).
What procedures are performed in your cath lab?
 Our cath lab and IR department performs approximately 150 procedures per week that includes the following:
Our cath lab and IR department performs approximately 150 procedures per week that includes the following:
- Left and right heart caths
- Myocardial biopsies
- Percutaneous coronary intervention (PCI)
- Intravascular ultrasound (IVUS)
- Fractional flow reserve (FFR [Boston Scientific and Volcano])
- Chronic total occlusions (CTOs)
- Intra-aortic balloon pumps (IABPs)
- Percutaneous ventricular assist devices (Impella [Abiomed])
- Rotablator rotational atherectomy (Boston Scientific)
- Diamondback orbital atherectomy (CSI)
- Structural heart procedures
- Patent foramen ovale (PFO)/atrial septal defect (ASD) closures
- Valvuloplasty
- Tempory pacemaker insertion
- Diagnostic and interventional peripheral angiograms (renal, runoffs, percutaneous transluminal angioplasty, and stenting)
- Transcatheter aortic valve replacement (TAVR)
- MitraClip (Abbott Vascular)
- Watchman (Boston Scientific)
- Extracorporeal membrane oxygenation (ECMO)
- Inferior vena cava (IVC) filter placement and removal
- Hepatic artery chemoembolization
- Radiofrequency ablation
- Transjugular intrahepatic portosystemic shunt (TIPS)
- Deep vein thrombosis (DVT) treatment
- Uterine and prostate artery embolization
Can you share more about your experience with TAVR?
 We performed our first TAVR case in 2011 and have since performed over 800 procedures. We started our program with a dedicated team of 2 RTs and 2 RNs, which allowed us to create the most consistent process and also further orient additional staff for these procedures. Currently, 75% of our staff are trained in TAVR procedures. We do not use surgical staff for these procedures unless a surgical cut down for access is required.
We performed our first TAVR case in 2011 and have since performed over 800 procedures. We started our program with a dedicated team of 2 RTs and 2 RNs, which allowed us to create the most consistent process and also further orient additional staff for these procedures. Currently, 75% of our staff are trained in TAVR procedures. We do not use surgical staff for these procedures unless a surgical cut down for access is required.
Do any of your physicians regularly gain access via the radial artery?
 Forty-nine percent (49%) of our procedures are performed using radial artery access.
Forty-nine percent (49%) of our procedures are performed using radial artery access.
Do any operators utilize pedal artery access when appropriate?
We do use pedal artery access when appropriate, and gain access using ultrasound and a pedal access kit.
Do you have cross-training? Who scrubs, who circulates, and who monitors?
 Yes, cross-training is an expectation in our department. Our staffing for each procedure room consists of 4 staff members. One RN is designated to circulate each case and one RT is designated to run the fluoroscopy machine. The other 2 staff could be a either RNs or RTs who can both scrub and monitor.
Yes, cross-training is an expectation in our department. Our staffing for each procedure room consists of 4 staff members. One RN is designated to circulate each case and one RT is designated to run the fluoroscopy machine. The other 2 staff could be a either RNs or RTs who can both scrub and monitor.
Are there licensure laws in your state for fluoroscopy?
 Yes, we follow the guidelines, protocol, and practices per Ohio Department of Health regulations. Only individuals who hold a valid Ohio radiologic license and physicians are able to administer fluoroscopy.
Yes, we follow the guidelines, protocol, and practices per Ohio Department of Health regulations. Only individuals who hold a valid Ohio radiologic license and physicians are able to administer fluoroscopy.
Which personnel can operate the x-ray equipment (position the image intensifier [II], pan the table, change angles, step on the fluoro pedal) in your cath lab?
 In our lab, we have a dedicated RT that moves the x-ray equipment, including positioning the II, panning the table, and stepping on the fluoroscopy pedal. We feel this has allowed us to minimize our radiation dosing to physicians, staff, and patients.
In our lab, we have a dedicated RT that moves the x-ray equipment, including positioning the II, panning the table, and stepping on the fluoroscopy pedal. We feel this has allowed us to minimize our radiation dosing to physicians, staff, and patients.
How does your cath lab handle radiation protection for the physicians and staff?
Every staff member is issued a lead apron, thyroid collar, and dose badge when they start in the department. Physicians will also use lead shin guards, radiation caps, and lead glasses. A radiation pad (SorbX, AngioSystems) and portable lead shields (used by the circulating RN) are used on every case to further protect against scatter radiation.
All lead pieces are inspected annually for defects and cleaned by staff when needed. We have recently partnered with Midwest Medical for protective lead products and use a tracking system they offer called Apron Tracker (Pulse Medical). Apron Tracker is a comprehensive, web-based, smart inventory management system for radiation protection products that has made inventory for lead products much easier.
What are some of the new equipment, devices and products recently introduced at your lab?
We recently switched over to the new Rotapro rotational atherectomy system (Boston Scientific) that allows the console and tank to be on one cart, and has easy-to-use controls incorporated on the advancer. We have intravascular lithotripsy (IVL) technology (Shockwave Medical) to treat calcified plaque in patients with peripheral artery disease. We also utilize the ClotTriever thrombectomy device (Inari Medical) and the FlowTriever retrieval and aspiration system (Inari Medical).
How does your lab communicate information to staff and physicians?
Our department has a team huddle every morning before the day begins to ensure all staff are aware of any issues or concerns for the day. We also have monthly staff meetings to communicate information to staff. We have implemented coordinators for the four main areas of growth in our departments: hybrid OR, critical limb ischemia (CLI), chronic total occlusions (CTOs) and interventional radiology. Our goal is that these coordinators will help with the communication among the physicians, managers, and staff.
Our hospital has implemented the use of Yammer (Microsoft), an enterprise social networking service used for private communication within organizations, to help communication not only in our department, but for overall hospital information as well.
How is coding and coding education handled in your lab?
We have two designated staff members for coding and American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) database abstraction. These two staff members review all documentation and make the necessary corrections for charging, coding, and ACC abstraction. Our coders attend a yearly seminar to keep up on any coding changes.
Where are patients prepped and recovered (post sheath removal)?
Our patients are prepped and recovered in our CardioVascular Recovery Unit (CVRU). This department pulls all our sheaths using manual pressure. Patients receiving closure devices, including Perclose (Abbott Vascular), Angio-Seal (St. Jude Medical), or Mynx (Cardinal Health), as well as TR Bands (Terumo), return to the CVRU post procedure.
How is inventory managed at your cath lab? Who handles the purchasing of equipment and supplies?
We currently use the PAR Excellence inventory system (PAR Excellence) to help with management of our supplies, ordering, and receiving, which is maintained by our inventory coordinator. Our inventory coordinator places all our orders for supplies and equipment needs, as well as receives and puts away the inventory when it arrives. A second shift senior supply distribution tech works 2:30pm-10:30pm to stock the procedure rooms for the next day’s procedures, as well as helps track and manage expired products.
Has your cath lab recently expanded in size and patient volume?
The cath lab and interventional radiology areas have both increased in patient volume over the last two years. Our interventional radiology department has enough increased volume to start inquiring about a second procedure room for them to use daily, thus allowing the cath lab to have an eighth procedure room.
Is your lab involved in clinical research?
We are very fortunate to partner with The Carl and Edyth Lindner Research Center at The Christ Hospital.
A few of the trials we are currently involved in include:
Aortic stenosis trials:
1. PARTNER 3 CAP: Low-risk TAVR/Sapien 3 (Edwards Lifesciences)
2. PARTNER 3 Valve-in-Valve: Stenosed bioprosthetic valve (Edwards Lifesciences)
3. RADIANT: High risk TAVR 24-26 mm (HLT Medical). Pending enrollment reopen
4. REPRISE EDGE: Intermediate- or high-risk TAVR (Lotus Edge, Boston Scientific)
5. EARLY TAVR: Asymptomatic critical aortic stenosis per “GXT Challenge” Sapien 3 vs surveillance (Edwards Lifesciences).
Heart failure with preserved ejection fraction (HFpEF) trial:
6. REDUCE-LAP-HF: InterAtrial shunt device (IASD) vs sham for reduction of left atrial pressure (Corvia Medical)
Peripheral arterial disease (PAD) trials:
7. TRANSCEND: SurVeil drug-coated balloon (DCB) provided “free” vs IN.PACT DCB in femoropopliteal percutaneous transluminal angioplasty (PTA) (Surmodics)
8. TOBA II BTK – Tack endovascular system for below-the-knee (BTK) PTA (non-randomized) dissections (Intact Vascular)
Percutaneous coronary intervention (PCI) trials:
9. PIONEER III: BuMA Supreme drug-eluting stent (DES) biodegradable polymer (Sino Medical Sciences Technology)
10. OPTIMIZE: Rapid exchange (RX) or integrated delivery system (IDS) DES with biodegradable polymer (Svelte Medical Systems) vs Promus (Boston Scientific)
11. EVOLVE 48: Synergy stent in 48 mm length, non-randomized (Boston Scientific)
Can you share your lab’s door-to-balloon (D2B) times and some of the ways employees at your facility have worked together to keep D2B times under the mandated 90 minutes?
We track this by median since we utilize the NCDR CathPCI metric in an effort to benchmark. From our latest outcomes report, which was 1Q2018, and published in 8/2018, our median D2B time for non-transfer ST-elevation myocardial infarction (STEMI) patients was 54 minutes (this is only for 1Q2018). Our rolling 4-quarter median D2B time was 60 minutes. The NCDR 50th percentile was 60 minutes.
Some of the Action Items we have worked on to improve D2B times are:
1) A collaborative initiative between the cath lab and emergency department (ED) to improve patient prep before arriving to the cath lab;
2) A monthly STEMI workgroup to discuss each STEMI case and time interval goals;
3) Working on developing processes for improving inpatient D2B times;
4) Collaborating with bed booking and admitting to enhance to ONE CALL/ activation process;
5) EMS performing training drills to identify process opportunities.
Who transports the STEMI patient to the cath lab during regular and off hours?
The cath lab staff (RN or RT) transports the patient to the lab with the RN from the ED during both on and off hours.
What do you do when the call team is already busy doing a procedure and a STEMI comes into the ED?
We call staff that are not being used on call to form another team to help.
What measures has your cath lab implemented in order to cut or contain costs?
The physicians, department management, and supply chain were able to collaborate on physician preference products so products aren’t being ordered off contract. We then determined what products the physicians wanted to use, without vendor input, and were able to negotiate aggressively. An example was moving from sole vendor in our lab to dual vendor in each product category vs a sole vendor for all products. We began this process by first limiting our vendor access, which prevented vendors from selling off-contract products, ensured commitment compliance and gave us greater negotiating power.
What quality control measures are practiced in your cath lab?
We perform STEMI reviews monthly with our quality department, hand washing technique quarterly, chart review monthly and we also follow-up with our post-op by rounding while they are in our post-op area and with a phone call after discharge.
How do you determine contrast dose delivered to the patient during an angiographic procedure?
We calculate the contrast load on each patient (GFR x 3.75) and this is discussed in the time out before each case is started.
Are you tracking the incidence of contrast-induced acute kidney injury (AKI) in patients?
We are currently tracking the high-risk patients and also those patients with a history of renal insufficiency.
How are you recording fluoroscopy times/dosages?
We record our fluoroscopy times and dosages on a daily log sheet and document these times in our patient procedure log. We also have the ability to attach the radiation dose report to our films in the Vericis system (HCA Technology Solutions).
The dosage we are using for documentation is:
- Fluoroscopy time (FT) greater than or equal to 40 minutes;
- Cine frames greater than or equal to 4500 total frames (cardiac: 15 fps) on a case OR greater than or equal to 900 frames on a case using digital runs (peripheral: anything exceeding 300 seconds of exposure);
- Air kerma (AK) greater than 3000 mGy.
What is the process that occurs if a patient receives a higher than normal amount of radiation exposure?
During the procedure, the physician is made aware of reaching more than 2 Gy in the current position or fluoro time above 40 minutes. We will also document this in the patient procedure log. Post procedure, the RT will fill out an Elevated Radiation report which includes fluoroscopy time (FT), cine frames for cardiac or peripheral, and air kerma, as well as the patient’s name, date of birth, medical record number, height, weight, physician, procedure room, and brief explanation of procedure (CTO, CLI, multiple vessels, etc.). The doses are recorded in a physician report and sent to our hospital’s radiation safety officer (RSO). The RSO computes the actual dosage in Roentgens on each patient and that information is sent to the performing physicians. The physician is responsible for follow-up with their respective patient.
Who documents medication administration during the case?
The RN documents medication administered during the case through Epic, as well as the staff who is monitoring documents in our Merge documentation system (IBM Watson Health). In November 2019, we will move to Epic’s Cupid module to cut down on double documentation.
Are your physicians dictating their cath procedure reports, or do they use a structured reporting tool?
Several physicians are using dictation to record procedure reports, but the majority use a template inside Epic to document procedure reports. We will move to structured reporting tool when we go live with Epic’s cardiac module, Cupid, in November 2019.
Do you use the American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) or any other outside data collection registry?
Yes, we use NCDR CathPCI and ACTION (Chest Pain-MI) registries.
How are you populating the registry data records?
There is a full-time employee (FTE) devoted to CathPCI data abstraction and also 1 FTE for ACTION (Chest Pain-MI). Consider the use of program coordinators (CLI and CTO coordinators) as they assist with collecting some of the data that is not within the registry. In our lab, we have two charge coders/data input specialists, and they initiate the process for STEMI patients by starting the record while the patient is still in-house. Our quality department completes the record and submits the data to the NCDR after the patient has been discharged.
How does your cath lab compete for patients?
We have grown our outpatient, urgent care and referral sites throughout the city of Cincinnati, which has allowed us to keep our volumes consistent. Also, partnering with the Lindner Research Center gives us the opportunity to offer our patients additional options that other hospitals in the city don’t have available.
How are new employees oriented and trained at your facility?
RTs and RNs attend one day of corporate orientation and the RNs attend an additional two days of network learning orientation prior to coming to the cath lab. Each new staff member is paired with their preceptor when they arrive to the lab. They start by reviewing their precept book and what needs to be completed before their orientation process is final, as well as review the schedule for the upcoming weeks.
Our orientation program is currently twelve to thirteen weeks for both RTs and RNs. RT orientation includes learning bi-plane x-ray (5-6 weeks), scrubbing coronary and peripheral procedures (4-5 weeks), and monitoring coronary and peripheral cases (2-3 weeks). RNs are paired with an RN preceptor for circulating (5 weeks), scrubbing coronary and peripheral procedures either with their current RN preceptor or an RT if needed (5-6 weeks), and finish with monitoring both coronary and peripheral procedures.
We utilize a variety of ways to train our staff. The primary training takes place within the lab performing procedures with their preceptor. We have vendors who assist with educational programs. For example, we have been able to offer an intra-aortic balloon pump (IABP) webinar with a hands-on review and utilize a cardiac catheterization book with assigned readings. We have didactic sessions for review of frequently used medications, coronary and peripheral anatomy, complications, and simulations for complications.
What continuing education opportunities are provided to staff members?
We block our schedule every other month for one hour to allow vendors to bring CEU opportunities to our staff. This past year, our physicians presented to staff on topics such as “How to be a good assistant for staff and physicians”, and we heard a testimonial from a patient that had a CTO procedure performed.
Are your clinical and/or managerial team members involved with any professional organizations that support the invasive cardiology service line, such as the Alliance for Cardiovascular Professionals (ACVP) or regional organizations?
Manager Mary Wagner is part of the
ACVP as well as the American Organization of Nurse Executives (AONE).The Assistant Manager, Bridget Spinney, is part of the ACVP, American Society of Radiologic Technologist (ASRT), and Ohio Society of Radiologic Technologists (OSRT).
How do you handle vendor visits to your lab?
We have a strict vendor policy that only allows vendors in the lab when requested by the physician for a specific procedure. Upon entry to the lab, vendors must have a valid RepTrax badge (machines available when you enter the hospital), and more recently, our vendors must have hospital scrubs (via a vendor scrub card to access scrubs through the hospital’s Cintas machine) to enter the procedure rooms. They must also have a red scrub cap on when entering the procedure room in order to be identified as a vendor. All vendors are to wait in the education room until the procedure starts or to be requested by the physicians.
Does your lab have a clinical ladder?
Our lab has clinical ladder for both the RNs and RTs.
Do you require your clinical staff members to take the registry exam for Registered Cardiovascular Invasive Specialist (RCIS)? Does staff receive an incentive bonus or raise upon passing the exam?
We do not require the staff to take the RCIS exam, but do highly recommend they complete it. We will reimburse the staff for the cost of the exam and for the cost of renewal.
Does your lab have any physical (layout) bottlenecks or limitations? How do you work around the resulting challenges?
Throughput in our Cardiovascular Recovery Unit (CVRU) continues to be a bottleneck area for our department. The input and output of patients is dependent on so many other areas or floors that we often see a backup in this area. We are also seeing an increase in interventional radiology procedures and without additional space for a second room, we are either working late in this area or we have a backup of patients who need to get procedures completed.
What do you like about the physical space in which you work?
We are located on the main floor of the hospital, making it accessible for our patients to valet and come right into our registration area and pre/post area.
Is there a particular mix of credentials needed for each call team?
Each call team has 4 staff members consisting of 2 RNs and 1 RT. The fourth staff member can either be an RT or RN. Most of our staff use the day after call as their day off.
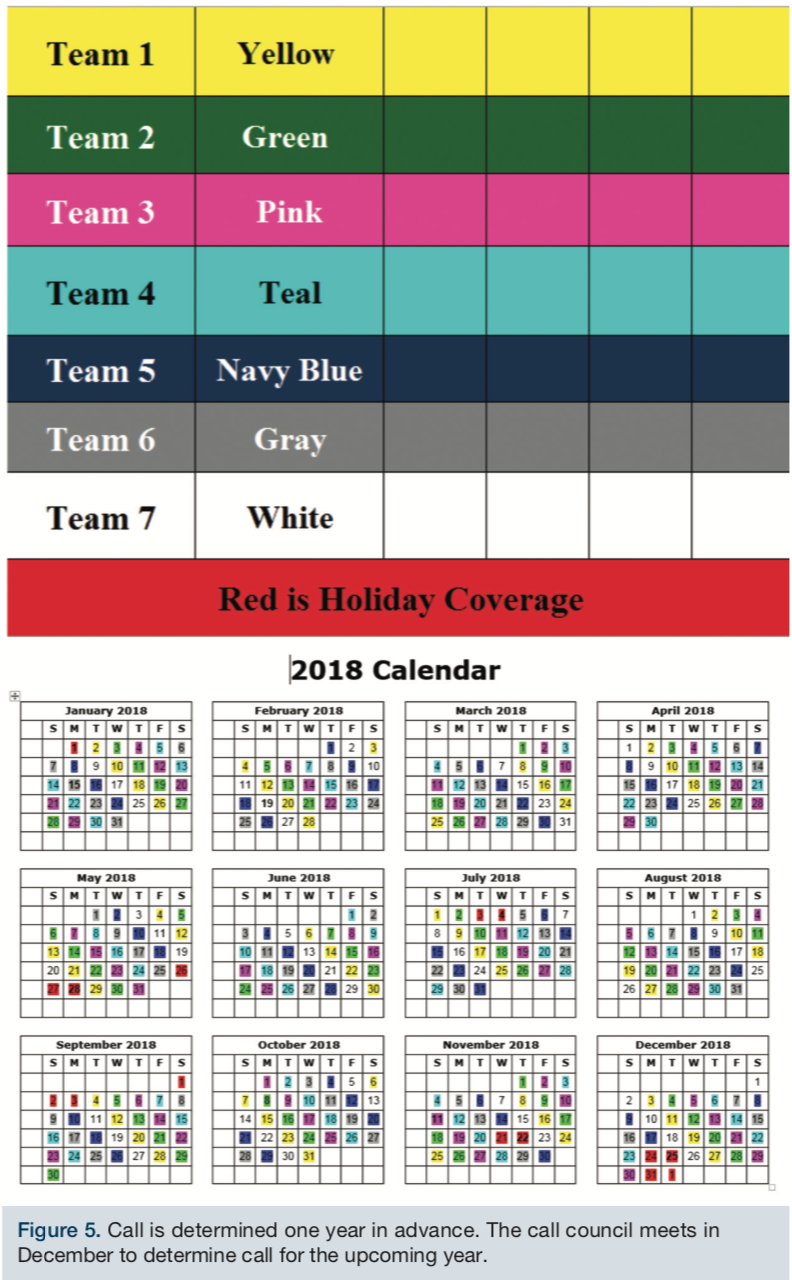
How does your lab schedule team members for call?
Our lab has a call council that help organize and designate the call teams, and which holidays each team is assigned. The call council members are in charge of posting any open call or delegating call when emergencies arise.
Our staff members are scheduled on call every 7th weekend in the cath lab and every 4th weekend in interventional radiology. Every year in December, the call council members meet and assign the call teams for the upcoming year. Call teams are assigned weekdays and weekends for the entire year. By assigning the call a year in advance, it has allowed our staff to be responsible for any trades or coverage on their own. When we have staff coverage issues such as medical leave, emergency situations and/or staffing issues, the call council takes care of posting call using a seniority list or emergency list, depending on the issue. Figure 5 is an example of our call team grid and calendar. Interventional radiology is similar, only with 4 call teams. Starting July 1, 2018, we implemented an evening shift (12:30pm-9:00pm) consisting of 2 RNs and 2 RTs. These staff members do not take call and this also allows us to finish up late cases for the day by not using our on-call staff, which was a staff satisfier in our department.
Within what time period are call team members expected to arrive to the lab after being paged?
Cath lab staff response time is 30 minutes and interventional radiology response time is 45 minutes.
Do you have flextime or multiple shifts? How do you handle slow periods?
Our staffing consists of 10-hour shifts from 7am-5:30pm and 12-hour shifts from 7am-7:30pm. We recently added an evening shift for Monday to Friday from 12:30pm-9:00pm consisting of 4 staff members (2 RNs and 2 RTs).
Do staff members have any particular perks that you might like to share?
Within our department, we have a mix of RN and RTs in the lab, so it was decided that we would combine Nurse Week and Radiologic Technologist Week into one big celebration week during National CardioVascular Technologist (CVT) week. It has brought our staff together for a common celebration and really built a sense of teamwork by celebrating everyone’s role in the lab.
Monthly, during our staff meeting, we recognize employees that were nominated by their peers for employee of the month. These staff members are recognized for going above and beyond to help their co-workers and patients.
Our staff currently get a three-hour minimum when called back and make time and a half when they get called back on call. This has been a huge staff satisfier in our department, because it allows them to go home early some days, but also make coming in on call worth the extra money. The staff also get free parking and have special parking when they get called in. Hospital-wide, staff can be nominated for the Daisy award and Smiles award.
Has your lab recently undergone a national accrediting agency inspection?
We have Ohio Department of Health (ODH), Joint Commission, and Magnet certification expected in 2019.
What trends have you seen in your procedures and/or patient population?
We are seeing an increased number of patients with co-morbidities. Our structural heart, ECMO, CTO, and CLI cases have also been on the rise.
What is unique or innovative about your cath lab and staff?
The greatest attributes of our staff include their flexibility in a quickly changing environment, and ability to attend to the complexity and volume of our cases.
Is there a problem or challenge your lab has faced?
Staffing and orientation are two challenges we face. We have a dedicated educator for our department that has allowed us to follow up on orientation plans, bridge gaps in staff training, and ensure new staff are getting what they need to complete orientation.
What’s special about your city or general regional area in comparison to the rest of the U.S.? How does it affect your “cath lab culture”?
We are very grateful to have the opportunity to partner with The Carl and Edyth Lindner Research Center at The Christ Hospital. As a result, we have been quickly introduced to many of the new techniques in cardiovascular medicine that have emerged over the past 25 years. These studies have included first-in-man as well as first-in-the-U.S. experiences with cutting-edge techniques.
A question from the American College of Cardiology’s National Cardiovascular Data Registry:
How do you use the NCDR Outcome Reports to drive quality improvement (QI) initiatives at your facility?
The NCDR CATH PCI and ACTION (Chest Pain-MI) data is reviewed at the patient level within the monthly Interventional Cardiology Quality Assurance Performance Improvement (QAPI) meeting, quarterly at the Heart and Vascular SL Quality and Patient Safety meeting, and annually at the Network QAPI. The data is reviewed in dashboard format, which allows us to view a trending analysis of historical and current outcomes. When downward trends are identified that are moving below the NCDR 50th percentile, the QAPI committee identifies that as an area of opportunity and will implement work-groups to discuss action plans as necessary. The work groups will report to the monthly Interventional Cardiology QAPI meeting with updates. n
Bridget Spinney, BRST, RT(R), can be contacted at bridget.spinney@thechristhospital.com. Mary Wagner, RN, BSN, NE-BC, can be contacted at mary.wagner@thechristhospital.com.
