


Advantage: Tirofiban in the Complex Puzzle of ACS Pharmacotherapeutics
Disclosure: Dr. Thomas Stuckey reports he is a consultant to Medicure.
Dr. Stuckey can be contacted at thomas.stuckey@conehealth.com.
Why did your hospital choose to create standard guidelines for the diagnosis and management of acute coronary syndromes (ACS)?
We believe it is important to have standard guidelines. It improves safety, and it also provides a platform encouraging the appropriate selections for optimal care. The guidelines we have put in place at our hospital serve as a map for most of the  providers. We have also worked as part of a bigger health system to coordinate across different facilities. For example, we work with the Carolinas Health System in Charlotte and several of its associated hospitals. We hold discussions frequently in order to try and adapt to various changes in practice. As long as you give the stakeholders a voice in the development of the guidelines, they generally will be on board with moving forward with that type of platform. The key is to attempt to create a platform that everyone can agree upon.
providers. We have also worked as part of a bigger health system to coordinate across different facilities. For example, we work with the Carolinas Health System in Charlotte and several of its associated hospitals. We hold discussions frequently in order to try and adapt to various changes in practice. As long as you give the stakeholders a voice in the development of the guidelines, they generally will be on board with moving forward with that type of platform. The key is to attempt to create a platform that everyone can agree upon.
Guidelines become an ongoing discussion, as you noted, but how long did it take to create an initial platform?
We spent about 6 months to a year talking about various approaches, and modify based upon changing studies and new outcomes that are determined in ongoing clinical trials.
Do you think most hospitals effectively adopt the current ACC/AHA/SCAI* guidelines?
Increasingly, the necessity of documenting outcomes has led to hospitals buying into following guidelines. We create modifications and adjustments to our protocols so that teams are well informed as to ongoing research changes that indicate a clinical change in practice.
Do you think most physicians are aware of the delayed onset of action of the newer P2Y12 inhibitors in STEMI patients?
This has been increasingly communicated over the past 6-12 months, so most interventional cardiologists are becoming aware of the data. First, it has been published. Second, the FDA has agreed to a labeling change that allows for crushed ticagrelor. That has improved the timing of onset of action.1
Are physicians aware of the delaying effect of morphine on onset of action of P2Y12 inhibitors?
There is one study2 that looks at clopidogrel action in normal controls, with and without morphine. Another study recently demonstrated the impact of morphine on both ticagrelor and prasugrel.3 It is now fairly well understood by most physicians providing STEMI care that morphine does delay the onset of action of P2Y12 inhibitors. How much that impacts the outcome is not always readily apparent to individual providers, but in general, there is an increasing understanding of the impact. In our institution, with the emergency room physicians in particular, we have discussed the interaction between morphine and the P2Y12 inhibitors. There has been an attempt by some providers to limit the use of morphine as a result, but this is obviously difficult in a struggling STEMI patient.
In your hospital’s guidelines, you recommend the use of GP IIb/IIIa inhibitors, specifically AGGRASTAT (tirofiban). When is this recommendation intended for use in ACS management?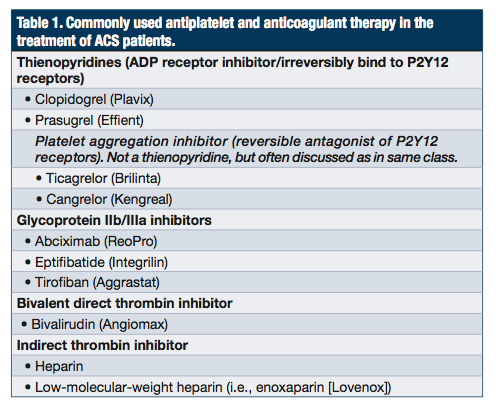
Our percutaneous coronary intervention (PCI) protocols are separately written for elective, unstable angina and non-STEMI, and STEMI populations. The use of tirofiban has been generally directed more toward the high-risk ACS population who have high thrombus burden. It is also recommended in those patients in whom we are unclear as to whether they have been able to receive an oral thienopyridine and keep it down.
What is the ACC/AHA/SCAI guideline recommendation for tirofiban and the other GP IIb/IIIa inhibitors?
The guidelines give a broad leeway to the individual provider as to how they want to use any of the available GP IIb/IIIa agents. We have chosen to use bivalirudin as our primary antithrombin agent, based on various pieces of information, at least in the STEMI population. The reduced bleeding from HORIZONS4 was confirmed in MATRIX5, as well as in BRIGHT6, and even though these data challenge the results of HEAT-PPCI7, the preponderance of evidence does favor bivalirudin, especially in patients who have a high risk of bleeding. However, along with bivalirudin use, there is a suggestion that an increased risk of acute stent thrombosis is present in the first 2-6 hours post procedure. As a result, based on the clinical situation, we have elected to incorporate the use of tirofiban as an option in our STEMI patients, particularly if there is a heavy thrombus burden or there are problems with the oral administration of a thienopyridine.
Why did your hospital choose tirofiban as the primary GP IIb/IIIa inhibitor, over other agents in the class, such as eptifibatide and abciximab?
From an economic standpoint, the high-dose bolus of tirofiban certainly is favorable, and it has received FDA approval. Furthermore, both clinical efficacy and safety data support its use.
Can you share some of the history of tirofiban leading up to the FDA’s approval of the high-dose bolus in late 2013?
In the early studies, the dosing turned out to be too low. Data shows that a higher degree of platelet inhibition is associated with better outcomes. The high-dose bolus tirofiban results in more potent platelet inhibition. That has gone along with the outcome data that is available, which ultimately led to the approval of tirofiban for this patient population.
In your hospital’s setting of PCI, tirofiban is administered using the high-dose bolus plus a short infusion. Why is a short (~2-6 hour) rather than a long (~12-18 hour) infusion of tirofiban used in this setting?
The longer infusion was historically based on convention. Part of the challenge is to try to balance the competing risks of ischemia and bleeding. With the newer oral thienopyridines, the onset of platelet inhibition is more rapid, so the infusion times can potentially be shorter, with potential reduction in bleeding. We certainly understand the importance of bleeding now and its influence on overall net outcome.
Why does the duration of the tirofiban short infusion depend on the P2Y12 agent selected?
One of the things that became obvious over the years is that the earlier the administration of a thienopyridine, the less robust the benefit of the GP IIb/IIIa inhibitors. However, with bivalirudin, there is an increased risk of acute stent thrombosis present in the first 2-6 hours after procedure completion. The discussion regarding the use of tirofiban has largely circled around trying to cover that so-called “vulnerable window” between the oral administration of the thienopyridine and when patients are fully platelet blocked. As the two newer, more potent agents, prasugrel and ticagrelor, have become available, it has become obvious that their onset of action is not as rapid in specific patient populations such as STEMI, where a variety of variables impair absorption and activation. In studies like FABOLUS PRO8, during that window of vulnerability, platelet inhibition is more robust with tirofiban. Do we need a glycoprotein inhibitor infusion for 18 hours? In the modern age of more rapid onset of the thienopyridines, that probably is no longer necessary. It just adds to bleeding risk.
Does your hospital use radial access?
Our radial access is approaching 70%. We have pushed that in the past two years. We are highly focused on bleeding avoidance strategies, which include developing a model for predicting what the bleeding risk is for each PCI case, predominantly favoring bivalirudin in patients who have the highest bleeding risk, and also favoring radial access whenever possible.
Are you tracking major and minor bleeds?
We track bleeding using the National Cardiovascular Data Registry (NCDR) definition, except in clinical trial protocols where BARC (Bleeding Academic Research Consortium), TIMI (Thrombolysis in Myocardial Infarction), and other definitions are added. We will adjust our protocols accordingly if we see a problem. In the last year, as part of our quality metrics, the biggest intervention that we have undertaken has been increasing our use and comfort levels with radial intervention. The benefit of radial access on bleeding risk has been documented in the MATRIX study as well.
Do you believe the clinical and safety benefits associated with radial access PCI allow the operator to use more aggressive antiplatelet therapy, especially in the high-risk ACS patient population?
I think that access site bleeding is less with radial access, but I don’t think it is necessarily eliminated, because not all bleeding is access site related. Let’s say a patient is seen in the emergency department (ED) and is able to receive heparin on the front end of the protocol. Our protocol calls for a 50 unit per kilo bolus with a maximum of 4000 units in the ED. In the heparin switch data from HORIZONS, there was not an increase in early stent thrombosis. If you look at the MATRIX data, the MATRIX patients received thienopyridines very early on in their course, and as a result, there was not a big increase seen in acute stent thrombosis. If a patient was able to receive early and timely administration of an oral thienopyridine such as ticagrelor, and received a heparin dose, then the likelihood of benefiting from a more aggressive antiplatelet strategy might only add to the risk. Alternatively, however, if you had a patient who arrived from the emergency medical services team, was placed on the cath lab table, and was vomiting, it might be unclear as to whether you were going to be able to get down a thienopyridine. Let’s also say there was no opportunity to give a heparin bolus up front and the patient had a large thrombus burden. In this patient, you might want to use an additional glycoprotein inhibitor. In ATLANTIC9, they gave an oral thienopyridine in the field versus giving it at the time of the procedure. Patients who received it in the field only had about a 30-minute lead time, but because of that 30-minute lead time, there was a significant reduction in the risk of stent thrombosis as a result of the administration of the oral thienopyridine. In that situation, by the time of the procedure, there is usually a reasonable level of antiplatelet activity and a GP IIb/IIIa inhibitor wouldn’t be necessary. But let’s say a patient was picked up at a Walmart 10 minutes away, brought to the cath lab, and was vomiting and had not received an oral thienopyridine. That is a situation where you don’t have much platelet activity on board at the time of your procedure and where an intravenous GP IIIb/IIIa inhibitor might help you.
Can you describe the transition to the tirofiban high-dose bolus regimen at your hospital?
We had very little trouble converting to tirofiban because our use of glycoprotein inhibitors was small to begin with and it was accompanied by excellent education within the cath lab itself, along with a discussion as to the benefits of making those changes. The whole process of making that transition went quite smoothly with our integrated service line.
Does use of the high-dose bolus of tirofiban add any additional time to the procedure?
No. We also have a pharmacist available for immediate interaction and help. For example, in the setting of STEMI, our pharmacist accompanies the patient to the cath lab. We have an excellent PharmD program and a very active team, who are all stakeholders and have all agreed on the protocols. The use of pharmacology in the cath lab is high enough (and the costs high enough) that close collaboration is required.
Have you been able to quantify any cost savings with tirofiban use as compared to the other glycoprotein IIb/IIIa inhibitors?
I don’t personally see the numbers, but the answer is pretty obvious. It is an important value play. We were a major HORIZONS-AMI trial enrollment site, so we have used predominantly bivalirudin and oral thienopyridines, and not used glycoprotein inhibitors, even though we did a lot of the glycoprotein inhibitor approval work in the early 1990’s. We had largely abandoned them in the last decade. Today, glycoprotein inhibitors have returned to our armamentarium as a result of unmet need and improved strategies to reduce bleeding risk.
Can you comment on some of the recent bivalirudin studies, such as HEAT-PPCI?
In our larger group of multiple hospitals where we talk quarterly, some of those facilities have adopted HEAT-PPCI. However, as we were developing the protocol, both the results of BRIGHT and the results of MATRIX were being presented. As I mentioned, it has been a moving target. However, due to the robust bleeding risk data and predictability of bivalirudin (avoiding repeated ACTs), bivalirudin has remained our agent of choice in STEMI patients. We also are going to trial the use of crushed ticagrelor as part of our strategies. We have also been discussing the possible administration of ticagrelor in the field to possible STEMI patients.
Recently the FDA approved Kengreal (cangrelor). Where do you think cangrelor will fit into your hospital’s guidelines for the diagnosis and management of ACS?
We were a site for the CHAMPION studies, conducted by The Medicines Company. Our cath lab team is used to administering cangrelor. There are a lot of issues, cost consideration being one of them, which may impact our decision to use or not use cangrelor. It does have desirable features that appeal to our team; specifically, immediate platelet inhibition, intravenous delivery, and quick reversibility.
The FDA, in their evaluation of cangrelor, noted a “window of vulnerability” that exists when transitioning a patient from cangrelor to a P2Y12 inhibitor. Should the “window of vulnerability” be a major concern for physicians?
Cangrelor is a drug that has rapid onset and rapid offset. When you administer it, it works immediately, and then after the procedure, it is continued for a couple of hours and then it is stopped. Clopidogrel cannot be administered until after the cangrelor is stopped, and clopidogrel doesn’t have its onset of action for a good 4-6 hours until after it is administered, so there is a so-called “window of vulnerability” where the platelets are not blocked. Ticagrelor can be used at any time during a procedure, so that window of vulnerability is substantially reduced by oral administration of ticagrelor during a procedure.
Any final thoughts?
Change is difficult, no matter how you institute it. But the current economic environment and service line integration is promoting better ability to change, especially when there are equivalent or even better therapies available. High-dose bolus tirofiban has been an excellent, cost-effective way to deal with patients who do not have optimal platelet inhibition at the time of PCI. It’s given us the flexibility to deal with that unmet need. n
References
- Parodi G, Xanthopoulou I, Bellandi B, Gkizas V, Valenti R, Karanikas S, et al. Ticagrelor crushed tablets administration in STEMI patients: the MOJITO study. J Am Coll Cardiol. 2015 Feb 10; 65(5): 511-512. doi: 10.1016/j.jacc.2014.08.056.
- Hobl EL, Stimpfl T, Ebner J, Schoergenhofer C, Derhaschnig U, Sunder-Plassmann R, et al. Morphine decreases clopidogrel concentrations and effects: a randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol. 2014 Feb 25; 63(7): 630-635. doi: 10.1016/j.jacc.2013.10.068.
- Parodi G1, Bellandi B2, Xanthopoulou I2, Capranzano P2, Capodanno D2, Valenti R2, et al. Morphine is associated with a delayed activity of oral antiplatelet agents in patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention. Circ Cardiovasc Interv. 2014 Dec 31;8(1). pii: e001593. doi: 10.1161/CIRCINTERVENTIONS.114.001593.
- Stone GW, Clayton T, Deliargyris EN, Prats J, Mehran R, Pocock SJ. Reduction in cardiac mortality with bivalirudin in patients with and without major bleeding: The HORIZONS-AMI trial (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction). J Am Coll Cardiol. 2014 Jan 7-14; 63(1): 15-20. doi: 10.1016/j.jacc.2013.09.027.
- O’Riordan M. MATRIX: Bivalirudin not superior to UFH on MACE end point in ACS, but benefits observed. Medscape: Conference News. March 20, 2015. Available online at https://www.medscape.com/viewarticle/841806. Accessed August 13, 2015.
- Han Y, Guo J, Zheng Y, Zang H, Su X, Wang Y, et al. Bivalirudin vs heparin with or without tirofiban during primary percutaneous coronary intervention in acute myocardial infarction: the BRIGHT randomized clinical trial. JAMA. 2015 Apr 7; 313(13): 1336-1346. doi: 10.1001/jama.2015.2323.
- Shahzad A, Kemp I, Mars C, Wilson K, Roome C, Cooper R, et al; HEAT-PPCI trial investigators. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. Lancet. 2014 Nov 22;384(9957):1849-58. doi: 10.1016/S0140-6736(14)60924-7.
- Valgimigli M, Tebaldi M, Campo G, Gambetti S, Bristot L, Monti M, Parrinello G, Ferrari R; FABOLUS PRO Investigators. Prasugrel versus tirofiban bolus with or without short post-bolus infusion with or without concomitant prasugrel administration in patients with myocardial infarction undergoing coronary stenting: the FABOLUS PRO (Facilitation through Aggrastat By drOpping or shortening Infusion Line in patients with ST-segment elevation myocardial infarction compared to or on top of PRasugrel given at loading dOse) trial. JACC Cardiovasc Interv. 2012 Mar;5(3):268-77. doi: 10.1016/j.jcin.2012.01.006.
- Montalescot G, van ‘t Hof AW, Lapostolle F, Silvain J, Lassen JF, Bolognese L, et al; ATLANTIC Investigators. Prehospital ticagrelor in ST-segment elevation myocardial infarction. N Engl J Med. 2014 Sep 11;371(11):1016-27. doi: 10.1056/NEJMoa1407024.
