


Cath Lab Spotlight: UnityPoint Health – Methodist
 UnityPoint Health – Methodist is one of 20 hospitals, 290 clinics, and 18 community network hospitals. UnityPoint Health provides care in 9 regions throughout Iowa, western Illinois, and southern Wisconsin. It is the nation’s 13th largest nonprofit health system and the fourth largest nondenominational health system in America. Our mission is to “Improve the health of the people and communities we serve” and our vision is “Best outcome, every patient, every time.” The cath lab at UnityPoint Health – Methodist is part of a service line that includes interventional cardiology, electrophysiology, echo, open heart surgery, and heart failure, and a cardiology physicians’ practice that includes all of the physicians necessary to support these services.
UnityPoint Health – Methodist is one of 20 hospitals, 290 clinics, and 18 community network hospitals. UnityPoint Health provides care in 9 regions throughout Iowa, western Illinois, and southern Wisconsin. It is the nation’s 13th largest nonprofit health system and the fourth largest nondenominational health system in America. Our mission is to “Improve the health of the people and communities we serve” and our vision is “Best outcome, every patient, every time.” The cath lab at UnityPoint Health – Methodist is part of a service line that includes interventional cardiology, electrophysiology, echo, open heart surgery, and heart failure, and a cardiology physicians’ practice that includes all of the physicians necessary to support these services.
We are located in the heart of Peoria, Illinois. There has been a “unification” with two other area hospitals, Proctor Community Hospital and Pekin Hospital. Our staff and physicians serve all 3 institutions.
What is the size of your cath lab facility and number of staff members?
 Our Methodist site consists of 4 procedure rooms: 2 cardiac labs (diagnostic and interventional), 1 electrophysiology (EP) lab, and 1 hybrid peripheral suite. The Proctor Community site has 2 cardiac labs (diagnostic and interventional) and 1 peripheral lab that is shared with the interventional radiology department. Pekin Hospital has 1 lab that performs diagnostic-only cardiac angiograms, and diagnostic and interventional peripheral studies. All 3 facilities have a pre and post recovery unit.
Our Methodist site consists of 4 procedure rooms: 2 cardiac labs (diagnostic and interventional), 1 electrophysiology (EP) lab, and 1 hybrid peripheral suite. The Proctor Community site has 2 cardiac labs (diagnostic and interventional) and 1 peripheral lab that is shared with the interventional radiology department. Pekin Hospital has 1 lab that performs diagnostic-only cardiac angiograms, and diagnostic and interventional peripheral studies. All 3 facilities have a pre and post recovery unit.
Our physician staff consists of 9 cardiologists, 1 cardiovascular surgeon, 1 independent cardiologist, 3 vascular surgeons, and 1 independent vascular surgeon. Cath lab staff includes 4 full-time critical care registered nurses (CCRNs), 4 PRN RNs, and 9 radiologic technologists (RT[R]s).
 Our staffing longevity is from 1-25 years of service IN the cath lab. We recently added up our years of service at Methodist (this includes our open-heart team). It was over 600 years.
Our staffing longevity is from 1-25 years of service IN the cath lab. We recently added up our years of service at Methodist (this includes our open-heart team). It was over 600 years.
All of our team members work in cardiac, peripheral, and implant procedures. Four of these team members work in the EP lab. Pre and post recovery is staffed with 3 RNs, who are part of the surgical prep and recovery department. We have 1 chaplain who assists daily with family updates and our patients’ religious needs. We also have 1 dedicated certified coder.
What procedures are performed in your cath lab?
 We have a vast array of cardiac procedures, including left and right heart catheterizations, and utilize fractional flow reserve (FFR), intravascular ultrasound (IVUS), intra-aortic balloon pumps (IABPs), Rotablator (Boston Scientific), and Impella (Abiomed). We also perform chronic total occlusion (CTO) procedures and stenting. Peripheral diagnostic and interventional procedures involve atherectomy, ELGs, hybrid procedures, carotid stenting, IVUS, radiofrequency (RF) ablations, fistula diagnosis, and interventions. Our implants include permanent pacemakers, implantable cardioverter defibrillators (ICDs), biventricular ICDs, and the Micra (Medtronic). Our EP team performs radiofrequency ablation of atrial fibrillation/flutter, ventricular tachycardia (VT), and premature ventricular contractions (PVCs), as well as cryoablation of supraventricular tachycardia (SVT). Some of our team also participates with the peripherally inserted central catheter (PICC) team. The PICC team consist of an all-RN team from both cath lab and open heart staff, and covers the Proctor and Methodist campuses.
We have a vast array of cardiac procedures, including left and right heart catheterizations, and utilize fractional flow reserve (FFR), intravascular ultrasound (IVUS), intra-aortic balloon pumps (IABPs), Rotablator (Boston Scientific), and Impella (Abiomed). We also perform chronic total occlusion (CTO) procedures and stenting. Peripheral diagnostic and interventional procedures involve atherectomy, ELGs, hybrid procedures, carotid stenting, IVUS, radiofrequency (RF) ablations, fistula diagnosis, and interventions. Our implants include permanent pacemakers, implantable cardioverter defibrillators (ICDs), biventricular ICDs, and the Micra (Medtronic). Our EP team performs radiofrequency ablation of atrial fibrillation/flutter, ventricular tachycardia (VT), and premature ventricular contractions (PVCs), as well as cryoablation of supraventricular tachycardia (SVT). Some of our team also participates with the peripherally inserted central catheter (PICC) team. The PICC team consist of an all-RN team from both cath lab and open heart staff, and covers the Proctor and Methodist campuses.
Does your lab perform primary angioplasty without surgical backup on site?
 The Methodist cath lab performs complex coronary and peripheral procedures with surgical staff backup on site. Methodist has 2 operating rooms and 24-hour coverage. The Proctor cath lab performs basic coronary and peripheral procedures. Pekin Hospital performs diagnostic coronary procedures only, but also does basic interventions for peripherals. Pekin and Proctor have an OR unit, but not open heart or vascular surgery. Critical patients are transferred to Methodist via Advanced Medical Transport (AMT) ambulance services.
The Methodist cath lab performs complex coronary and peripheral procedures with surgical staff backup on site. Methodist has 2 operating rooms and 24-hour coverage. The Proctor cath lab performs basic coronary and peripheral procedures. Pekin Hospital performs diagnostic coronary procedures only, but also does basic interventions for peripherals. Pekin and Proctor have an OR unit, but not open heart or vascular surgery. Critical patients are transferred to Methodist via Advanced Medical Transport (AMT) ambulance services.
What is your rate of normal diagnostic catheterizations?
 The average rate of normal diagnostic caths is 1000 a year.
The average rate of normal diagnostic caths is 1000 a year.
Do any of your physicians regularly gain access via the radial artery?
Yes, there are 3 coronary physicians who routinely gain radial access for ST-elevation myocardial infarction (STEMI) and non-STEMI procedures. Radial procedures are performed on 45% of our coronary percutaneous coronary intervention (PCI) cases and approximately 65% of diagnostic cases.
If you are performing peripheral vascular procedures, do any operators utilize pedal artery access when appropriate?
All of our vascular surgeons and 1 interventional cardiologist will obtain pedal access as needed for complex vascular cases. These are usually ultrasound and/or Doppler guided.
Who manages your cath lab?
Alexander Adler, MD, FACC, FHFSA, is our medical director. He is board-certified in internal medicine, cardiovascular disease, and heart failure transplantation. Tina Miller, RN, MSN, MBA, NEA-BC, is the Executive Director of Cardiovascular Integrated Services. Shannon Glover, RN, BSN, manages the cath labs, except for the Pekin campus. She also manages open heart at Methodist and the care unit at the Proctor campus, as well as the PICC team for both campuses. She is overseeing and consulting for the Pekin campus at this time, which is currently going through UnityPoint Health integration.
Do you have cross-training? Who scrubs, who circulates and who monitors?
RT(R)s routinely rotate between scrubbing and monitoring roles. RNs mostly circulate. Our patient care team will always have 1 RN and 1 RT(R) to scrub, and 1 of either license to monitor.
Are there license laws in your state for fluoroscopy?
Yes, the state of Illinois has a government body called the Illinois Emergency Management Agency (IEMA). Illinois law states only licensed personnel can operate radiologic imaging equipment.
Certified RT(R)s must complete 24 hours of continuing education biannually in order to maintain licensing.
Which personnel can operate the x-ray equipment (position, pan the table, change angles, step on the fluoro pedal) in your cath lab?
The RT(R)s and physicians.
How does your cath lab handle radiation protection for the physicians and staff?
The hospital has a governing Radiation Safety Committee and Radiation Safety officer. There is 1 quality control RT(R) that maintains badge and exposure reporting. She oversees the radiation equipment testing by a physicist, and tracks lead aprons and their annual testing for Methodist and Proctor campuses. We also have a dedicated RT(R) who serves on the committee and assists her in the cath labs for lead testing.
New team members are fitted for wraparound aprons, thyroid shielding, lead glasses, and protective hats, if wanted. Sterile RadPads (Worldwide Innovations & Technologies, Inc.) are provided on all cases. The Pekin cath lab has a senior RT(R) who handles radiation protection for that campus. All staff that work in our area are expected to do a yearly NetLearning competency test on ALARA (“as low as reasonably achievable”).
How is coding and coding education handled in your lab?
We have charge forms geared to each procedure and a dedicated coder. She performs coding for cath lab and open-heart procedures at Methodist and Proctor. She has 19 years of coding experience and is a certified professional coder (CPC) through the AAPC, with 18 required hours of continuing education per year. She does a presentation every year at a staff meeting to update or clarify coding issues. We are certainly fortunate to have her.
Who pulls the sheaths post procedure, for both interventions and diagnostic procedures?
The RT(R)s, nurses, and physicians pull for diagnostic and intervention. There is mandated observation by senior personnel for new staff for their first 5 sheath pulls. They are then able to pull sheaths themselves. All nurses and scrub RT(R)s are trained on closure devices and post procedure care. Outpatients are transferred to our recovery area. Inpatients are transferred to the cardiovascular intensive care unit (CVICU) or to our step down cardiac unit, where staff is trained on access management. Closure devices are deployed by the physicians. Manual pulling can be done in the lab or the patient can be taken to another patient care area for pulling. It depends on caseload volume and needed procedure flow.
What are some of the new equipment devices and products recently introduced at your cath lab?
We have instantaneous wave-free ratio (iFR, Philips), Aquamantys bipolar sealers (Medtronic), Resolute Onyx stents (Medtronic), Surfacer (Bluegrass Vascular Technologies), the leadless pacemaker Micra (Medtronic), and the Impella (Abiomed). We have just completed a new state-of-the-art EP lab that is using an esophageal temp probe (Circa Scientific) and EnSite Precision Cardiac Mapping System (Abbott).
The SpaceTRAX inventory system (Stanley Healthcare) was added to the Proctor campus for better inventory control. A new Witt hemodynamic monitoring system (Philips) was also installed at Proctor in order to standardize procedure documentation and increase staff competency. Stryker reprocessing has been added to the cath lab for EP catheters.
How does your lab communicate information to staff and physicians to stay on top of change?
Our coder performs two roles. One is coding and the second role is answering phones. Daily, we have a rotating “board runner”. They communicate case changes and delays to physicians and cath lab staff. Both people keep procedure flow going for all 3 campuses.
The department manager makes case assignments the day before and posts them, so people know which campus to go to and the cases they will be doing for the day.
Our cases are posted on a large board in our main hallway, with color coding of the physicians. This is another way of keeping physicians and staff updated for add-ons and time changes.
Our manager sends daily emails (huddle notes), and organizes monthly staff meetings and quarterly meetings, including 1 meeting for the RNs, 1 for RT(R)s, 1 for open heart, and one for the care unit. She also attends a monthly physician meeting.
We have “reminders” put on flip chart paper and posted inside our bathroom stalls.
Our break room has multiple dry erase boards and bulletin boards on every wall that are geared specifically to certain topics, e.g., engagement, wellness classes at our gym, birthdays, and our favorite, THE POT LUCK!
Our monthly meetings include guest speakers and vendors. It is a time we also receive policy reviews or updates. Most staff members serve on a hospital committee or project and will share updates regarding their assignment.
How is inventory managed at your cath lab?
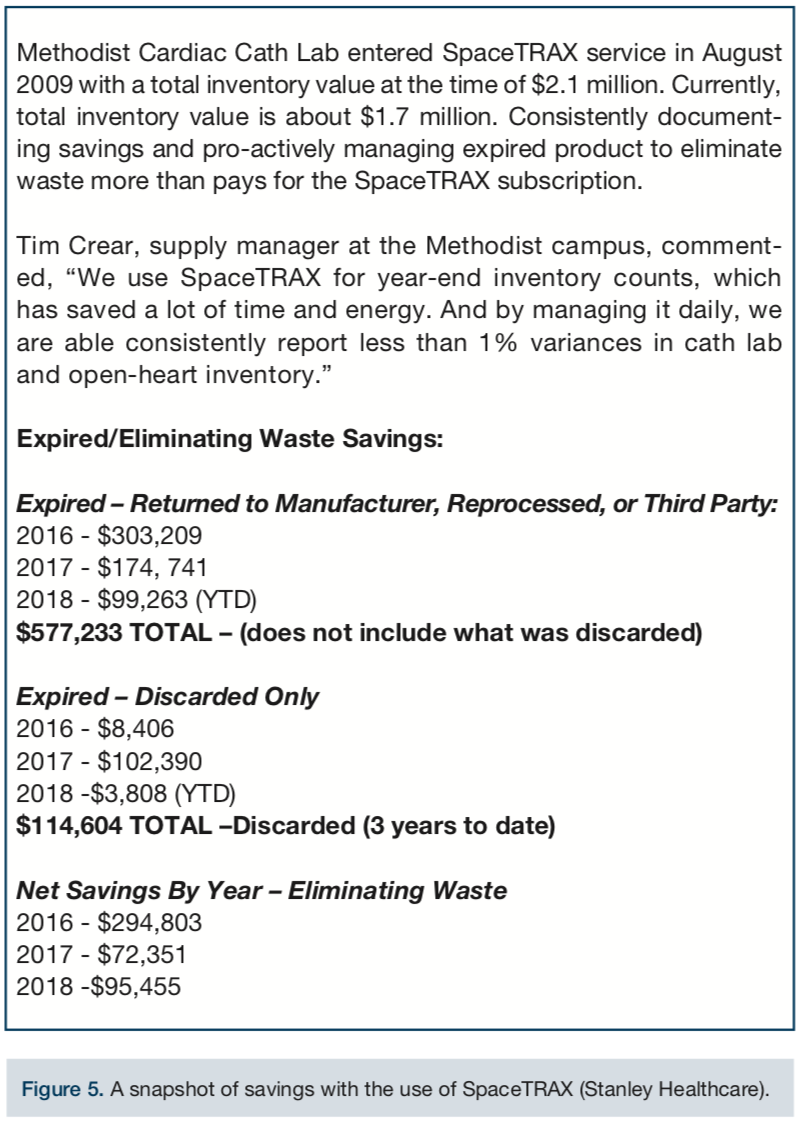
SpaceTRAX is our electronic inventory management tool at UPH Methodist and Proctor (Figure 5). It shows us inventory usage, physician procedure costs, expired product, and what should be reordered. All staff are trained at different tiers for SpaceTRAX utilization.
There are 4 team members at the Methodist and Proctor campuses that will receive product from the warehouse, check it into SpaceTRAX, and put it away. There are 3 requesters who can initiate equipment purchases under our manager’s supervision. They also do this in between patient care assignments. It is a constant, never-ending process in our lab.
Methodist has a central supply department that handles daily miscellaneous supply stocking: syringes, saline, etc. This is also being initiated at Proctor. Pekin is currently manually counting supplies, but looking to purchase SpaceTRAX in 2018.
Where are patients prepped and recovered (post sheath removal)?
All three campuses have a prep and recovery area that is skilled and specific to the cath lab. It is staffed with RNs that are trained to address our patients’ specific needs. They perform:
- Prep: start an IV, shave, dress, consent, check for current labs, and history & physical;
- Post care: sheath pulling, monitoring access site, patient and family education, and discharge;
Cardioversions, loop recorder insertions, and transesophageal echocardiograms (TEEs) are also performed in this unit.
Has your cath lab recently expanded in size and patient volume?
The Methodist campus now has 2 EP labs; a new cath/EP lab was just completed. The new lab has allowed us to increase our efficiency and better serve our patient population by being able to perform 2 ablations a day. We are currently integrating with Pekin Hospital and its cath lab.
Is your lab involved in clinical research?
The Methodist campus is participating in the Surfacer Research Study (Evaluation of the Surfacer System Approach to Central Venous Access).
Can you share your lab’s average door-to-balloon (D2B) times and some ways employees have worked together to keep D2B times under the mandated 90 minutes?
Our average D2B time is 72 minutes at Methodist. Proctor is 78 minutes. All of Pekin’s STEMI patients are transferred to Methodist by paramedics, so they are included in the Methodist time window for transfers.
When patients present in the emergency department (ED) with chest pain, an electrocardiogram (EKG) is done within 10 minutes. There are 3 cath lab call personnel and 1 STEMI physician on call 24/7. Labs are drawn in the ED, and an IV and drugs started. The patient is then transported directly to the cath lab. The city’s emergency medical services (EMS) personnel are able to communicate with the ED and send an EKG for suspected STEMIs. This allows for calling/paging the call team and beginning room/procedure preparedness for the patient’s arrival.
A STEMI task committee meets monthly, and reviews fallouts and ways to improve times. We are working on an internal D2B time of 60 minutes to increase proficiency. We are also registered with the American Heart Association’s Mission: Lifeline.
Who transports the STEMI patient to the cath lab during regular and off hours?
STEMI patients are transferred by ED staff and we are given handoff information.
What do you do when the call team is already busy doing a procedure and a STEMI comes to the ED?
The cath lab has everyone’s phone numbers posted. If need be, volunteers are asked to come in and given shift bonus for their time. When absolutely necessary, a patient procedure will be abandoned and moved to the CVICU, or their staff will come and stay with a patient so the STEMI can be addressed. If we know late or long procedures are going to run after hours, a volunteer backup call team for STEMIs is implemented. This happens infrequently.
What measures has your cath lab implemented to reduce costs?
We utilize our electronic system’s information for par levels. We will share products among the three campuses to reduce “overall” spending due to caseload variances. Our inventory requesters review individual items for discontinuing or par level reduction monthly when reviewing expiration and reordering reports. We have been able to shift some items to consignment instead of owned. Contracted bulk buys have been used when possible that allow us a reduction in dollars spent or will allow for needed equipment inclusion. Being part of a larger, 9-hospital unit helps us to work with vendors to reduce unit prices. Also, the ACIST CVi contrast injection system is utilized in most of our procedures by several physicians. This can also be set up for low viscosity mixes. Our expired product is donated to third-world organizations.
What quality control measures are practiced in your cath lab?
There are monthly acute MI/STEMI data review meetings that review fallouts. Also, there are quarterly cath PCI reviews with physicians on their data. There are audits performed on all complications and reviews are done with physicians as needed.
How are you recording fluoroscopy times and doses?
We have dose timing tracked on all our units. This is transposed to our patient procedure report.
Any dose that is in excess of 5Gy is reported by the RN into our RL Solutions software, and a radiation oncology nurse and next caregiver are notified. The patient is followed up at 2, 4, 6, 8, and 12 weeks. These cases are reviewed by our radiation safety officer and at risk management meetings. The operating physician is notified every 5 minutes and when they reach 3Gy. Dosing and time are displayed on procedure monitors at all times.
How do you determine contrast dose delivered to the patient during angiographic procedures?
The ACIST CVi injector gives us an exact amount. If low viscosity contrast media is used, the ACIST amount is times 0.7. Colored syringes and labeling stickers are used on the sterile field to help staff keep track of hand injections. Manual eyeballing is used for manifold procedures.
Are you tracking the incidence of contrast-induced acute kidney injury in patients?
Pre-procedure labs must be done within 30 days of the angiogram and rehydration is scheduled if necessary. Doses are documented in the patient procedure report and the operating physicians state the amount in their dictation. Physicians define patient care and follow-up. This data is also tracked in the National Cardiovascular Data Registry (NCDR) CathPCI registry per provider.
Who documents medication administration during the case?
The RN documents in the monitoring system during the case. This is shared with the next caregiver for their handoff forms.
Are physicians dictating their cath procedure reports or do they use a structured reporting tool?
The structured tool is available for them, but our operators dictate their procedure report. They also chart an immediate post procedure note in Epic.
Do you use the American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) or any other outside data collection registry?
Yes, we participate in the NCDR CathPCI registry. This data self-populates through the Philips hemodynamic system. We have 3 data abstractors focused on registry data, and their focus is divided as follows: the NCDR ICD Registry: 1 abstractor; NCDR Peripheral Vascular Intervention (PVI) Registry: 1 abstractor; NCDR AFib Registry: 1 abstractor – done by analytics dept; and CathPCI Registry: 3 abstractors. We also participate in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) Registry and the NCDR ACTION Registry (now the Chest Pain – MI Registry), and those are handled by our analytics department.
How are new employees oriented and trained at your facility?
New staff have a week of hospital orientation that includes policies and expected standards and values. In the department, new employees have a mentor/call buddy for 90 days for basic skills. They meet with our manager frequently to discuss orientation needs, progress, and goal setting. Everyone is sent to ECG, basic life support (BLS), and advanced cardiovascular life support (ACLS) classes. We have a large orientation manual for each license that is read by each new employee. It is up to the manager if longer orientation time is needed.
How is staff competency evaluated?
All staff have yearly competencies and review their job description. Our manager gives everyone a yearly job performance evaluation that is also attached to their pay increase. She uses staff and physician input, as well as her own observation. We also have computer-based training required through NetLearning that must be met. There are yearly comps on equipment and procedures. We review our ACLS practices, defibrillators, and so on.
What continuing education opportunities are provided to staff?
Continuing education is done by vendors for new equipment and supplies. Quarterly inservices are done by vendors on more infrequent supplies like the Impella, Rotablator, etc., to keep current the wide range of skills needed by staff. Staff is also sent to symposiums and conferences to enhance their job knowledge. American Society of Radiologic Technologists (ASRT) membership is provided to keep our CEUs for RT(R)s. Physicians, other hospital representatives, and vendors attend monthly staff meetings and share information on devices and topics such as right heart catheterizations, etc.
How do you handle vendor visits to your lab?
Vendors are required to schedule time in advance. They must meet RepTrax requirements and wear the badge at all times. They are also expected to wear a red surgical hat. If a vendor is invited by a physician to come for a procedure, this is also acceptable.
Do you require your clinical staff to take the registry exam for the registered cardiovascular invasive specialist (RCIS) credential? Does staff receive an incentive bonus or raise on passing the exam?
No, all staff must be licensed, but it can be RN or RT(R). We do have a RT(R) who took the RCIS exam and passed. The RCIS review and test is paid for by Methodist.
Tell us about your department’s physical space.
We have limited square footage. We have remodeled and upgraded our x-ray equipment in 3 of our 4 rooms at Methodist and 1 room at Pekin over the last 5 years. These procedure rooms are improved, but we have met a lot of physical limitations. We also share our work area with 2 open-heart rooms. Between the cath lab and open-heart supplies, we need more storage space. We are very landlocked at this time.
How does your cath lab handle call time for staff members?
We have 1 call team for everything, everywhere. It is 1 RN and 2 RT(R)s. Staff chose this instead of 2 call teams to improve their work/life balance. Their call can be hectic, but they have more off time. This has not impacted patient care. There is 1 STEMI call doctor, so they are hectic together. Staff typically have 1 set weekday call and 1 weekend a month. The call team has 30 minutes to arrive after being paged.
Do staff members have any little or big particular perks that you might like to share?
Staff has paid ASRT membership. Self-scheduling is allowed as long as cases are covered. Paid time off (PTO) is not required for low census, but is still an option. We have flexibility with appointments and family obligations, such as changing hours to fit with work/life balance. There are monthly birthday and work anniversary celebrations. We receive recognition if we are mentioned by name on a patient survey at staff meetings. Our manager will also celebrate above and beyond efforts with our peers. She is also able to give “shout-outs” recognizing staff and other department members at intra-department manager meetings. Team-building parties are scheduled off campus twice a year with our greater work family, including the CVICU and step down unit.
Do you have flextime or multiple shifts? How do you handle slow periods?
Most staff work four to five 8-hour shifts a week. Two RT(R)s work four 10-hour shifts.
During low census, the manager will post “things to do” such as checking expirations, NetLearning, comps, room cleaning, etc. There is an option to go home early. Several staff have additional duties: inventory, PACS, and NCDR data collection. They always have something to do.
Are your clinical or managerial team members involved with any professional organizations that support the invasive cardiology service line?
Our manager participates in Association of periOperative Registered Nurses (AORN) and is a Society for Cardiovascular Angiography and Interventions (SCAI) member.
Has your lab recently undergone a national accrediting agency inspection?
Yes, we underwent Joint Commission accreditation in 2017 and Illinois Department of Public Health (IDPH) in 2017.
What trends have you seen in your procedures and/or patient population?
We are using different access sites: radial, pedal, brachial, subclavian, antegrade, and cut downs. Many of our patients have more than 1 co-morbidity. We do a lot of abdominal aortic aneurysm (AAA) grafts. The Midwest diet, manufacturing, and farming exposure risks impact certain population groups. Our EP procedures have expanded in the last 5 years and this has increased our EP caseload.
Is there a problem or challenge your lab has faced?
Yes, construction woes and physician shortages (we have only 1 cardiovascular surgeon and 2 interventional cardiologists). We always have staffing holes due to medical reasons or vacations. There is not enough equipment storage space, and we have some older equipment that is or will be needing updating.
Where is your cath lab located in relation to the OR and ED?
The Methodist work area was designed to keep cardiac care close together. Two open-heart suites share our immediate work space. Our progressive unit and CVICU are directly beyond our double-entry doors. Our prep/recovery area is 1 floor above us. The Methodist ED is in the same hospital wing, but 2 floors down. We have a “code blue” elevator that accommodates rapid transportation. The Proctor ED is on the same floor as the cath lab, and they do not have open-heart backup on campus. The patient is transferred to the appropriate facility. The Pekin ED and cath lab are on the same floor.
What is unique or innovative about your cath lab and staff?
There has been a combined effort among physicians, anesthesia, scheduling, and staff schedules to accomplish a workflow that better meets case volume needs. For example, some doctors have blocked scheduling days/times. Staff themselves developed 1 call team between the Methodist and Proctor cath labs. This decreased their call hours, decreased call pay to the hospital, and gave staff satisfaction because of fewer individual call days per month. This also increased productivity and decreased overall labor cost. Some of our open-heart RNs have cross-trained to circulate cases in the cath lab to help with staffing holes.
Our staff has a wide age range, from the mid 20s to the mid 60s. We trialed 10-hour days for staff. The four people who trialed it have stated it is the best thing they have ever done. They like the work-life balance it offers and this schedule has also decreased the overtime budget, since they are on regular time to finish cases that run after hours. Their days off are alternated, so there are four full teams to cover. Some staff trialed going from an 80-hour pay period to a 72- or 64-hour pay period in order to have a day off, decrease burnout, and improve work-life balance. Every staff member who made that change has not gone back to their previous hours. PRN people are utilized for staff openings. Our manager considers the use of PRNs to be a wonderful option, because they are not here all the time, they are always happy, and being content keeps them competent as well. Our manager is very approachable in regard to trying new ideas and new ways of doing things that “have always been done this way”. She believes “happy staff = happy patients”.
What is special about your city or general regional area in comparison to the rest of the United States?
Peoria is a river city in central Illinois. It is set along the Illinois River with a population of 115,000 people. It was settled in 1680 by French explorers. We are home to Caterpillar, Inc., and local colleges, including Bradley University, Illinois Central College, and Midstate Technical Institute. Our city council has developed a warehouse district that has a museum, concerts, restaurants, night entertainment, and a baseball diamond. It is along the waterfront and hosts many festivals year round. There is a St. Jude research facility at another institution. The region has several wineries, craft distilleries, and a wildlife state park. The river is used for recreation and transportation of goods. There is also a replicate paddle boat that offers cruises. The Paradise casino also resides on the river. Peoria is an industrial city surrounded by smaller communities and farmland. It has a lot to offer fishermen and hunters, and has lots of other outside activities. There are a lot of smaller communities to live in if you don’t like the city life. There is a large 4th of July fireworks display sponsored by UnityPoint Health - Methodist. We are only a couple of hours from Chicago, St. Louis, and our state capital, Springfield, all offering even more cultural and sports activities close by. Peoria is also the home of Richard Pryor, Dan Fogelberg, Gary Richrath (REO), Sam Kinison, Jim Thome, Shaun Livingston, and Bob Michel.
A note from author Sally Weiman, RT(R): “I have worked in the cath lab for almost 20 years. Our technology has changed! Smaller catheters, leadless pacemakers, transcatheter aortic valve replacement (TAVR), digital processing — it is fascinating when you think about it. I have loved the victories. It makes you feel like a rock star. I still remember the name of the first patient we lost. My team cried with her family. The cath lab really is a calling, a service to humanity, a gift to our community. I am proud to be a part of it.”
Shannon Glover, RN, Department Manager, can be contacted at shannon.glover@unitypoint.org.
Sally Weiman, RT(R), Coronary Specialist, Inventory Coordinator, can be contacted at sally.weiman@unitypoint.org.
